



Chronic abdominal pain in children: could it be IBS?
“Mom, dad, my tummy hurts…”. Just an excuse to skip school, or a real illness? If the abdominal pain is recurrent (more than 4 days a month, for more than two months), it may be irritable bowel syndrome, or IBS.
Let’s dispel a few misconceptions from the outset. No, IBS isn’t just in the child’s head: it’s a real, recognized disorder. No, it’s not caused by a poor diet, although certain dietary imbalances can make it worse. No, it’s not the parents’ fault. No, it’s not a serious illness, and it’s certainly not cancer.
Now that we’ve covered those points, how can you recognize the symptoms? When should you see a healthcare professional? What solutions are available? The answers are below.
Healthcare professionals section
Find here your dedicated section
About this article




Definition, epidemiology, symptoms and diagnosis
What is IBS in children?
IBS is a disorder of intestinal function that cannot be explained by any identifiable abnormality (lesion, disease, etc.) 1,2. In short, everything seems fine in young Louise’s stomach, but she really is in pain.
What distinguishes abdominal pain caused by IBS from other types of stomach pain? First, its recurrence: more than 4 days a month, for more than two months. But that’s not all: the symptoms are linked to bowel movements and/or a change in stool frequency and/or appearance (Rome IV criteria 3).
Is your teenager Raphaël often constipated, but you’re not sure if it’s IBS or functional constipation? It’s actually quite simple: if he has IBS, the pain will not go away when the constipation episode ends 2.

What impact does IBS have on the child’s life and the family?
Although not life-threatening, IBS has a significant impact on children’s quality of life: missed school days, difficulty concentrating and remembering things, giving up sports, social isolation, low self-esteem, sleep disorders and fatigue, to name but a few.
The entire family unit is disrupted, whether emotionally (severe anxiety), economically (cost of treatment, sleep deprivation of parents and impact of medical appointments on their work) or in terms of daily life (giving up certain activities, time spent on diagnosis and treatment) 2,4,5,6.
IBS in children greatly impacts the parents’ professional lives: loss of parental work productivity accounts for nearly a quarter of the cost of care in the European Union. 2
1 in 20 children are affected
Louise and Raphaël are far from being isolated cases. Globally, it is estimated that one in nine children suffer from a functional abdominal disorder, and that one in 20 children suffer specifically from IBS, the most common subtype of these disorders in children 7.
Young Asians may be more affected than Europeans or Americans, but the difference remains slight and may be explained simply by different interpretations of diagnostic criteria 7.
5.8 % Worldwide prevalence of irritable bowel syndrome. ⁷
Risk factors
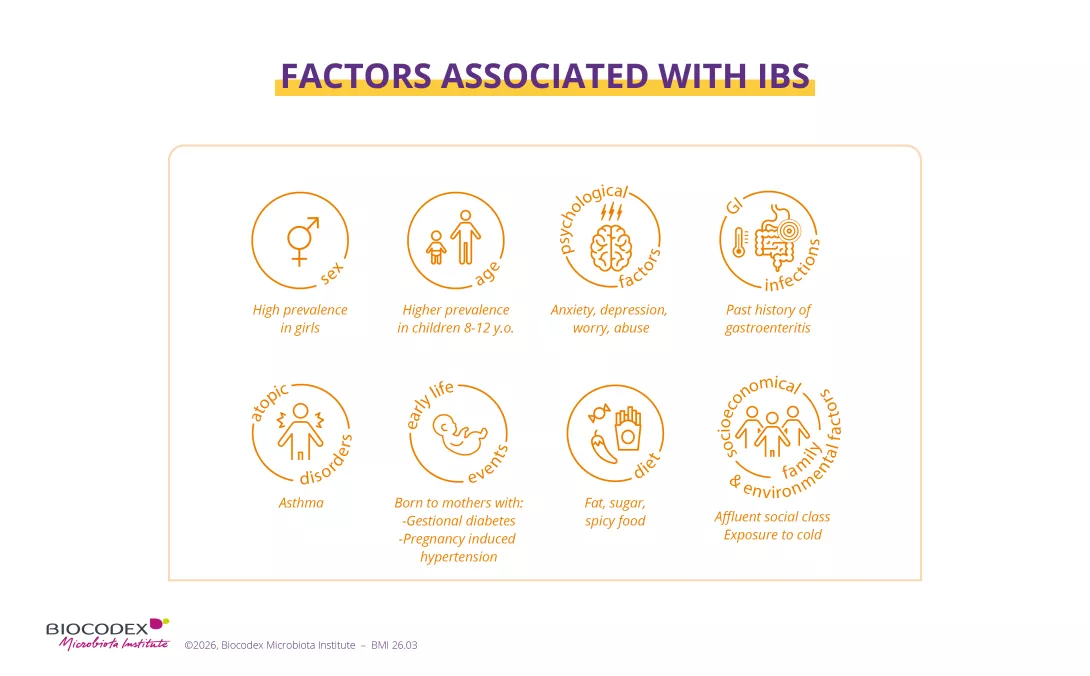
But above all, in the case of both Louise and Raphaël, IBS is more likely to be the result of a combination of factors, starting with psychological ones (anxiety about school or relationships, difficult experiences, etc.), which can make a child more susceptible to abdominal pain.
Has Louise suffered from gastrointestinal infections such as gastroenteritis, or food allergies? Does Raphaël enjoy foods that are too fatty, too spicy or too sweet? This could trigger or worsen their symptoms 2.


The challenge of diagnosis in children
Because there are no specific biomarkers, diagnosis of IBS in children, as in adults, is based on the assessment of clinical symptoms 2,8.
But here lies the first obstacle: symptoms vary from one child to another, to the extent that IBS has been classified into four subtypes.
Other difficulties might include young Louise struggling to describe her symptoms or teenager Raphaël feeling embarrassed to talk about them, while their parents may over- or under-interpret their child’s words depending on their stress or personal experience, increasing the risk of underdiagnosis.
Finally, there are undeniable cultural differences in the perception of pain and intestinal transit 2,8.
Therefore, while IBS is the most common functional gastrointestinal disorder in children, its complex diagnosis often means a long, difficult and expensive experience for families.
Subtypes of irritable bowel syndrome (IBS) and their diagnostic criteria according to the Rome IV criteria:
More than a quarter (25%) of stools are classified as severe constipation (hard, difficult-to-pass lumps) or mild to moderate constipation (lumpy, sausage-shaped stools), and less than a quarter (25%) as mild diarrhea (fluffy pieces with ragged edges, a mushy stool) or severe diarrhea (watery stools with no solid pieces).
More than a quarter (25%) of stools are classified as mild diarrhea (fluffy pieces with ragged edges, a mushy stool) or severe diarrhea (watery stools with no solid pieces), and less than a quarter (25%) as severe constipation (hard, difficult-to-pass lumps) or mild to moderate constipation (lumpy, sausage-shaped stools).
More than a quarter (25%) of stools are classified as severe constipation (hard, difficult-to-pass lumps) or mild to moderate constipation (lumpy, sausage-shaped stools), and more than a quarter (25%) as mild diarrhea (fluffy pieces with ragged edges, a mushy stool) or severe diarrhea (watery stools with no solid pieces).
Patients who meet diagnostic criteria for IBS but whose bowel habits cannot be accurately categorized into one of the three groups above.
IBS subcategories are very important in the management of affected children. 2

Where does this pain come from? What science says today
The origin is still very unclear
The mechanisms behind pediatric functional abdominal disorders in general, and IBS in particular, remain poorly understood in 2025. The prevailing theory suggests that IBS results from a disruption of the gut-brain axis 9.
Two mechanisms have been proposed 2 :
- The top-down model suggests that the disorder begins in the brain: Louise’s symptoms may be triggered by her anxiety, as her brain sends abnormal signals to her gut causing pain, bowel problems and changes in the gut microbiota;
- The bottom-up model suggests that everything begins in the gut: Louise’s disorder may have been triggered by a gastrointestinal infection that sent pain alert messages to the brain.
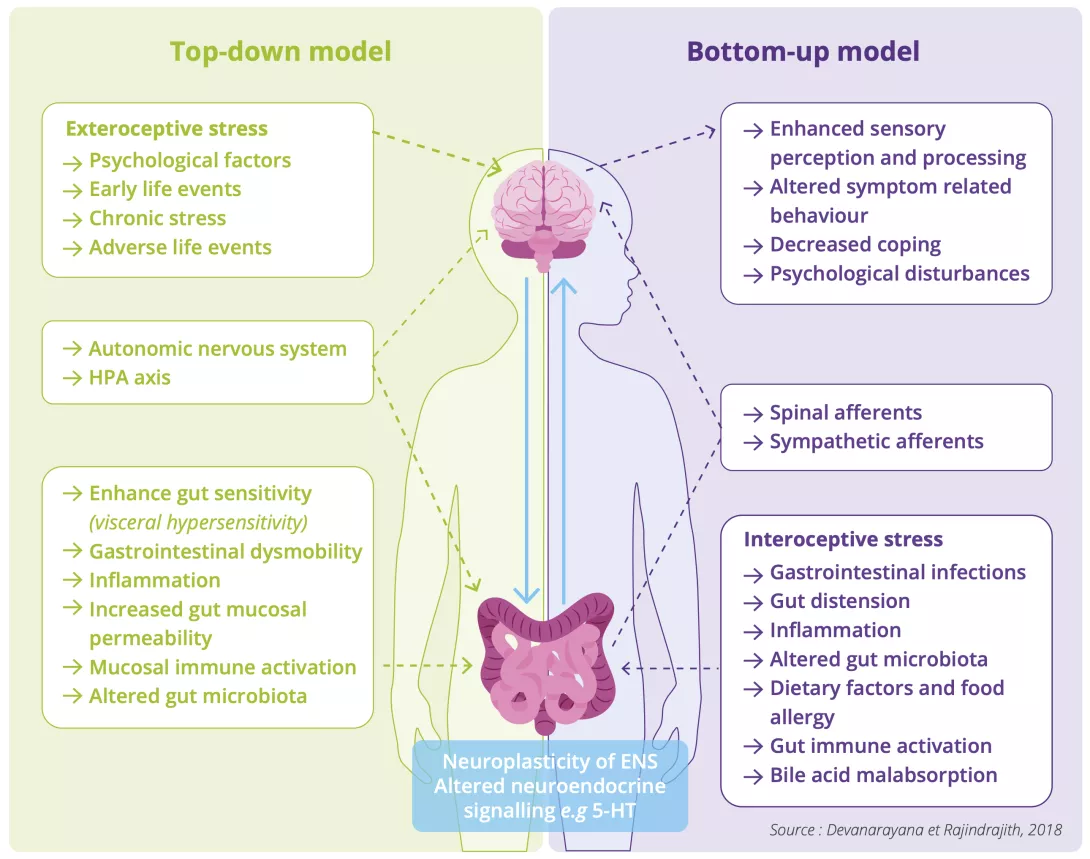
While both mechanisms will likely coexist (bidirectional interaction between the brain and the gut) in Louise once the disorder is established, it remains difficult to know which one initiated it 2.

The microbiota: just one piece of the puzzle
Whether it is the cause (bottom-up model) or the consequence (top-down model) of Louise’s IBS, the gut microbiota is now a major line of research. Several factors explain this interest:
- Louise’s gut microbiota influences her digestion, immunity and gut-brain communication;
- it is less diverse and some bacteria are more prevalent: this imbalance is called dysbiosis 2,10,11;
- a simple transfer of Louise’s microbiota to microbiota-free mice is enough to trigger symptoms in the rodents (visceral sensitivity, changes in bowel function, etc.) 2.
Nevertheless, IBS remains a multifactorial condition: gut flora is just one piece of a much more complex puzzle.

“Over the past decade, particular attention has been paid to the gut microbiota, which is believed to play a key role in IBS.”



Further studies are still needed, particularly in children, to confirm the role of the gut microbiota and, perhaps one day, to establish a profile of the gut bacteria associated with the disorder, or even to identify the “microbial signature” specific to each child in order to tailor treatment accordingly 2. This is because the treatment Louise needs is not the same as that needed by Raphaël.
What this means for parents
The gut microbiota can therefore serve as a possible tool 12 as part of a personalized, multidisciplinary therapeutic approach 2,8.
A high-fiber diet and use of specific probiotics (to support beneficial bacteria) or antibiotics (to kill pathogenic bacteria) are strategies that could help Louise or Raphaël, always under medical supervision 8,9.

How can we help a child with IBS?
From diagnosis to treatment decisions
Effective management of Louise’s IBS requires an accurate diagnosis: detailed medical history (background, medications, social and psychological factors) and a physical examination to rule out organic disorders 2,8.
The IBS subtype (is Louise’s IBS constipation-predominant, diarrhea-predominant, mixed or unclassified?) must be identified as it will guide the therapeutic approach and the personalization of treatment over time 2,8.
Once the diagnosis has been made, Louise and her family must work together with the medical team to make decisions: close communication between the child, family and medical staff improves treatment success.
Education should focus on the nature of the diagnosis, the relevance of the connection between the gut and brain, the effects of lifestyle and other triggers, and an outline of potential treatment approaches and options. 13
Multidisciplinary management
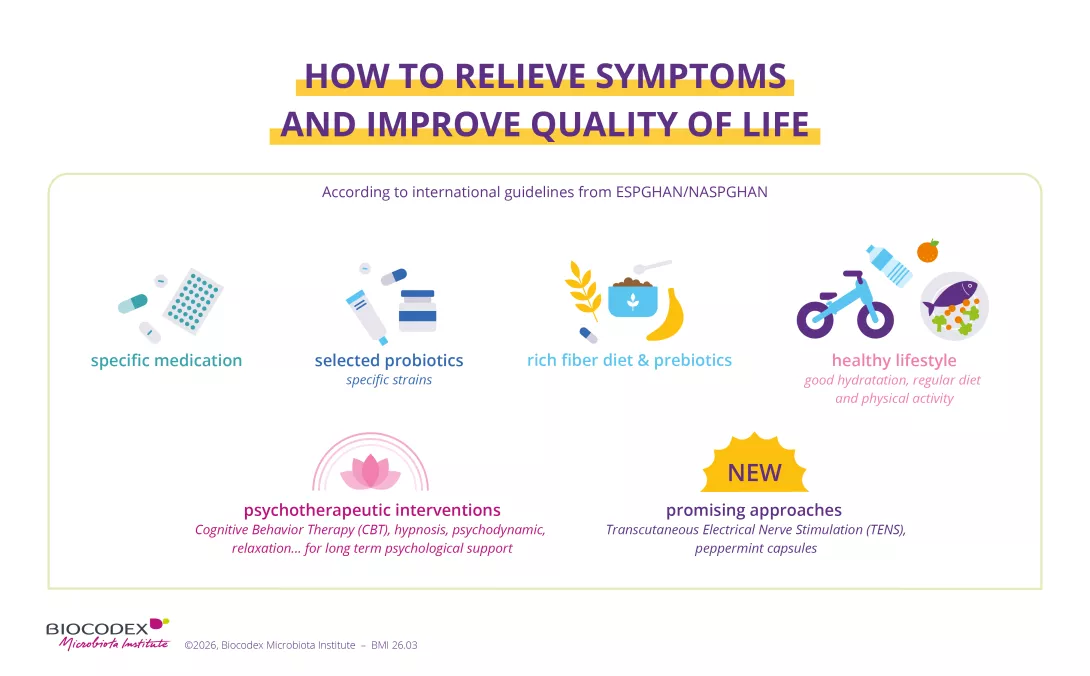
Approaches combining multiple therapies, in addition to any medication strategies, deliver the best results 2, 5, 8, 13 :
- Psychology: communication and dialogue between child, parent and clinician 13
- Hypnotherapy (home-based or otherwise) 14, cognitive behavioral therapy (CBT), neurostimulation 13
- Nutrition: a personalized, child-centered approach incorporating advice from a dietitian, promoting fiber intake and avoiding age-inappropriate restrictive diets 13
- Probiotics, and more specifically lactobacilli such as Lactobacillus rhamnosus GG 5, 13 or L. reuteri 4, and prebiotics to selectively feed the good bacteria;
- Healthy lifestyle: physical exercise, sleep consistency.
Management of children with IBS may include either non-pharmacological (diet, psychologic interventions, specific fibers and probiotics) and pharmacological strategies (PEG, rifaximin, antispasmodics, gut-brain neuromodulators), as long as they are individualized to the patient’s symptoms, often entailing a multidisciplinary approach. 8


Avoid:
- self-medication and/or dosages and durations exceeding local recommendations (e.g., repeated use of laxatives);
- vicious cycles: parental anxiety, which increases as the child’s symptoms worsen, can undermine treatment. 2
IBS is diagnosed by a doctor or pediatrician. They can assess the situation, reassure your child and recommend appropriate treatment. If your child experiences frequent abdominal pain, talk to a healthcare professional. They can guide you to the most suitable solutions.
Patients stories: living with Irritable Bowel Syndrome (IBS)
Warning signs requiring prompt medical attention
- Family history of chronic inflammatory bowel disease, celiac disease or peptic ulcer
- Persistent right-sided abdominal pain
- Difficulty swallowing or pain when swallowing
- Persistent vomiting
- Gastrointestinal bleeding
- Nighttime diarrhea
- Arthritis
- Sores or fissures around the anus
- Unintentional weight loss
- Slowed statural growth
- Delayed puberty
- Unexplained fever
1. Vermeijden NK, de Silva L, Manathunga S, et al Epidemiology of Pediatric Functional Abdominal Pain Disorders: A Meta-Analysis. Pediatrics. 2025 Feb 1;155(2):e2024067677. doi: 10.1542/peds.2024-067677.
2. Devanarayana NM, Rajindrajith S. Irritable bowel syndrome in children: Current knowledge, challenges and opportunities. World J Gastroenterol. 2018 Jun 7;24(21):2211-2235. doi: 10.3748/wjg.v24.i21.2211.
3. Rome Foundation. Appendix A: Rome IV Diagnostic Criteria for FGIDs. Available from: https://theromefoundation.org/rome-iv/rome-iv-criteria/. [Last concult: 2026 Jan 20]
4. Romano C, Ferrau' V, Cavataio F, Iacono G, Spina M, Lionetti E, Comisi F, Famiani A, Comito D. Lactobacillus reuteri in children with functional abdominal pain (FAP). J Paediatr Child Health. 2014 Oct;50(10):E68-71. doi: 10.1111/j.1440-1754.2010.01797.x.
5. Kianifar H, Jafari SA, Kiani M, et al. Probiotic for irritable bowel syndrome in pediatric patients: a randomized controlled clinical trial. Electron Physician. 2015 Sep 16;7(5):1255-60. doi: 10.14661/1255.
6. Vernon-Roberts A, Alexander I, Day AS. Systematic Review of Pediatric Functional Gastrointestinal Disorders (Rome IV Criteria). J Clin Med. 2021 Oct 29;10(21):5087. doi: 10.3390/jcm10215087.
7. Vermeijden NK, de Silva L, Manathunga S, Spoolder D, Korterink J, Vlieger A, Rajindrajith S, Benninga M. Epidemiology of Pediatric Functional Abdominal Pain Disorders: A Meta-Analysis. Pediatrics. 2025 Feb 1;155(2):e2024067677. doi: 10.1542/peds.2024-067677.
8. Di Nardo G, Barbara G, et al. Italian guidelines for the management of irritable bowel syndrome in children and adolescents : Joint Consensus from the Italian Societies of: Gastroenterology, Hepatology and Pediatric Nutrition (SIGENP), Pediatrics (SIP), Gastroenterology and Endoscopy (SIGE) and Neurogastroenterology and Motility (SINGEM). Ital J Pediatr. 2024 Mar 14;50(1):51. doi: 10.1186/s13052-024-01607-y.
9. Gordon M, Sinopoulou V, Tabbers M et al. Psychosocial Interventions for the Treatment of Functional Abdominal Pain Disorders in Children: A Systematic Review and Meta-analysis. JAMA Pediatr. 2022 Jun 1;176(6):560-568. doi: 10.1001/jamapediatrics.2022.0313.
10. Saulnier DM, Riehle K, Mistretta TA et al. Gastrointestinal microbiome signatures of pediatric patients with irritable bowel syndrome. Gastroenterology. 2011 Nov;141(5):1782-91. doi: 10.1053/j.gastro.2011.06.072.
11. Hollister EB, Oezguen N, Chumpitazi BP, et al. (2019). Leveraging Human Microbiome Features to Diagnose and Stratify Children with Irritable Bowel Syndrome. J Mol Diagn. 2019 May;21(3):449-461. doi: 10.1016/j.jmoldx.2019.01.006.
12. Baştürk A, Artan R, Yılmaz A. Efficacy of synbiotic, probiotic, and prebiotic treatments for irritable bowel syndrome in children: A randomized controlled trial. Turk J Gastroenterol. 2016 Sep;27(5):439-443. doi: 10.5152/tjg.2016.16301.
13. Groen J, Gordon M, Chogle A, et al. ESPGHAN/NASPGHAN guidelines for treatment of irritable bowel syndrome and functional abdominal pain-not otherwise specified in children aged 4–18 years. J Pediatr Gastroenterol Nutr. 2025 Aug;81(2):442-471. doi:10.1002/jpn3.70070.
14. Rutten JMTM, Vlieger AM, Frankenhuis C et al. Home-Based Hypnotherapy Self-exercises vs Individual Hypnotherapy With a Therapist for Treatment of Pediatric Irritable Bowel Syndrome, Functional Abdominal Pain, or Functional Abdominal Pain Syndrome: A Randomized Clinical Trial. JAMA Pediatr. 2017 May 1;171(5):470-477. doi: 10.1001/jamapediatrics.2017.0091.
See also





